What is mammography?
 Mammography is a specific type of imaging that uses a low-dose x-ray to examine breasts. A mammography exam, called a mammogram, is used to aid in the early detection and diagnosis of breast diseases in women.
Mammography is a specific type of imaging that uses a low-dose x-ray to examine breasts. A mammography exam, called a mammogram, is used to aid in the early detection and diagnosis of breast diseases in women.
Three recent advances in mammography include digital mammography, computer-aided detection and breast tomosynthesis.
Digital mammography, also called full-field digital mammography (FFDM), is a mammography system in which the x-ray film is replaced by solid-state detectors that convert x-rays into electrical signals. These detectors are similar to those found in digital cameras. The electrical signals are used to produce images of the breast that can be seen on a computer screen or printed on special film similar to conventional mammograms. From the patient’s point of view, having a digital mammogram is essentially the same as having a conventional film mammogram.
Computer-aided detection (CAD) systems use a digitized mammographic image that can be obtained from either a conventional film mammogram or a digitally acquired mammogram. The computer software then searches for abnormal areas of density, mass, or calcification that may indicate the presence of cancer. The CAD system highlights these areas on the images, alerting the radiologist to the need for further analysis.
Breast tomosynthesis, also called three-dimensional (3-D) breast imaging, is a mammography system where the x-ray tube moves in an arc over the breast during the exposure. It creates a series of thin slices through the breast that allows for improved detection of cancer and fewer patients recalled for additional imaging.
-
What are some common uses of the procedure?
Mammograms are used as a screening tool to detect early breast cancer in women experiencing no symptoms. It can also be used to detect and diagnose breast disease in women experiencing symptoms such as a lump, pain or nipple discharge.
-
Screening mammography
Mammography plays a central part in early detection of breast cancers because it can show changes in the breast up to two years before a patient or physician can feel them. Research has shown that annual mammograms lead to early detection of breast cancers, when they are most curable and breast-conservation therapies are available.
-
How should I prepare?
Before scheduling a mammogram, discuss any new findings or problems in your breasts with your doctor. In addition, inform your doctor of any prior surgeries, hormone use, and family or personal history of breast cancer.
Do not schedule your mammogram for the week before your period if your breasts are usually tender during this time. The best time for a mammogram is one week following your period. Always inform your doctor or x-ray technologist if there is any possibility that you are pregnant.Do not wear deodorant, talcum powder or lotion under your arms or on your breasts on the day of the exam. These can appear on the mammogram as calcium spots.
Describe any breast symptoms or problems to the technologist performing the exam.
If possible, obtain prior mammograms and make them available to the radiologist at the time of the current exam. Ask when your results will be available; do not assume the results are normal if you do not hear from your doctor or the mammography facility. -
What does the equipment look like?
 A mammography unit is a rectangular box that houses the tube in which x-rays are produced. The unit is used exclusively for x-ray exams of the breast, with special accessories that allow only the breast to be exposed to the x-rays. Attached to the unit is a device that holds and compresses the breast and positions it so images can be obtained at different angles.
A mammography unit is a rectangular box that houses the tube in which x-rays are produced. The unit is used exclusively for x-ray exams of the breast, with special accessories that allow only the breast to be exposed to the x-rays. Attached to the unit is a device that holds and compresses the breast and positions it so images can be obtained at different angles. -
How is the procedure performed?
During mammography, a specially qualified technologist will position your breast in the mammography unit. Your breast will be placed on a special platform and compressed with a paddle (often made of clear Plexiglas or other plastic). The technologist will gradually compress your breast.
Breast compression is necessary in order to:
· Even out the breast thickness so that all of the tissue can be visualized.
· Spread out the tissue so that small abnormalities are less likely to be obscured by overlying breast tissue.
· Allow the use of a lower x-ray dose since a thinner amount of breast tissue is being imaged.
· Hold the breast still in order to minimize blurring of the image caused by motion.
· Reduce x-ray scatter to increase sharpness of picture.You will be asked to change positions between images. The routine views are a top-to-bottom view and an angled side view. The process will be repeated for the other breast.
You must hold very still and may be asked to keep from breathing for a few seconds while the x-ray picture is taken to reduce the possibility of a blurred image. The technologist will walk behind a wall or into the next room to activate the x-ray machine.
When the examination is complete, you will be asked to wait until the radiologist determines that all the necessary images have been obtained.
The examination process should take about 30 minutes.
-
What will I experience during and after the procedure?
You will feel pressure on your breast as it is squeezed by the compression paddle. Some women with sensitive breasts may experience discomfort. If this is the case, schedule the procedure when your breasts are least tender. Be sure to inform the technologist if pain occurs as compression is increased. If discomfort is significant, less compression will be used.
-
Who interprets the results and how do I get them?
A radiologist, a physician specifically trained to supervise and interpret radiology examinations, will analyze the images and send a signed report to your primary care or referring physician, who will discuss the results with you. You will also be notified of the results by the mammography facility.
Follow-up examinations may be necessary, and your doctor will explain the exact reason why another exam is requested. Sometimes a follow-up exam is done because a suspicious or questionable finding needs clarification with additional views or a special imaging technique. A follow-up examination may also be necessary so that any change in a known abnormality can be monitored over time. Follow-up examinations are sometimes the best way to see if treatment is working or if an abnormality is stable over time.
-
What are the benefits vs. risks?
Benefits:
· Imaging of the breast improves ability to detect small tumours. When tumours are small, there are more treatment options.
· The use of screening mammography increases the detection of small abnormal tissue growths confined to the milk ducts in the breast, called ductal carcinoma in situ (DCIS). These early tumours cannot harm patients if they are removed at this stage and mammography is the only proven method to reliably detect these tumours. It is also useful for detecting all types of breast cancer, including invasive ductal and invasive lobular cancer.
· No radiation remains in a patient’s body after an x-ray examination.
· X-rays usually have no side effects in the typical diagnostic range for this exam.Risks:
· There is always a slight chance of cancer from excessive exposure to radiation. However, the benefit of an accurate diagnosis far outweighs the risk.
· The effective radiation dose for this procedure varies.
· False Positive Mammograms. 5 percent to 15 percent of screening mammograms require more testing such as additional mammograms or ultrasound. Most of these tests turn out to be normal. If there is an abnormal finding, a follow-up or biopsy may have to be performed. Most of the biopsies confirm that no cancer was present. It is estimated that a woman who has yearly mammograms between ages 40 and 49 has about a 30 percent chance of having a false-positive mammogram at some point in that decade and about a 7 percent to 8 percent chance of having a breast biopsy within the 10-year period.
· Women should always inform their physician or x-ray technologist if there is any possibility that they are pregnant. -
A word about minimizing radiation exposure
Special care is taken during x-ray examinations to use the lowest radiation dose possible while producing the best images for evaluation. National and international radiology protection organizations continually review and update the technique standards used by radiology professionals.
Modern x-ray systems have controlled amount of x-ray beams and dose control methods to minimize stray (scatter) radiation. This ensures that those parts of a patient’s body not being imaged receive minimal radiation exposure. -
What are the limitations of Mammography?
Initial mammographic images themselves are not usually enough to determine the existence of a benign or malignant disease with certainty. If a finding or spot seems suspicious, your radiologist may recommend further diagnostic studies.
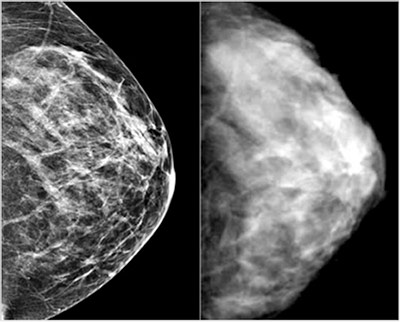
Interpretations of mammograms can be difficult because a normal breast can appear differently for each woman. Also, the appearance of an image may be compromised if there is powder or salve on the breasts or if you have undergone breast surgery. Because some breast cancers are hard to visualize, a radiologist may want to compare the image to views from previous examinations. Not all breast cancers can be seen on mammography.
Women with dense and small breast may not fully benefit the Mammography procedure as it would not provide reliable results.
Breast implants can also impede accurate mammogram readings because both silicone and saline implants are not transparent on x-rays and can block a clear view of the tissues behind them, especially if the implant has been placed in front of, rather than beneath, the chest muscles. Experienced technologists and radiologists know how to carefully compress the breasts to improve the view without rupturing the implant.
When making an appointment for a mammogram, women with implants should ask if the facility uses special techniques designed to accommodate them. Before the mammogram is taken, they should make sure the technologist is experienced in performing mammography on patients with breast implants.
While mammography is a good screening tool for breast cancer available today, mammograms do not detect all breast cancers. Also, a small portion of mammograms indicate that a cancer could possibly be present when it is not (called a false-positive result).
Research is being done on a variety of breast imaging techniques that can contribute to the early detection of breast cancer and improve the accuracy in distinguishing non-cancerous breast conditions from breast cancers. Among them is a 3D Breast Ultrasound option. For more information, please visit www.canadianbreastscreening.com